Any person could walk past Marie Marsden and believe they know her story. Dressed in distressed jeans, a beige woven tank top and four inch heels with a purse draped over her shoulder, she seems like any other woman traveling through life’s daily work and social routines. What makes Marsden different is the medical device she has attached to her heart—a Left Ventricular Assist Device (LVAD), a machine attached to her 24 hours a day, used to help her heart pump blood throughout her body. Marsden, the mother of two, was diagnosed with post-partum dilated cardiomyopathy (PPCM), “a rare, life-threatening heart disease of unclear origin and is characterized by heart failure of sudden onset between the final weeks of pregnancy and six months after delivery,” according to the National Institute of Health. This heart patient believes she was recently discriminated against by an Indianapolis Metropolitan Police Department sergeant. She said the officer told her she was prohibited from parking in a “handicapped spot” despite the placard hanging from her rear view mirror. Marsden told the Indianapolis Recorder Newspaper during the incident, which she stated took place in the parking lot of Kilroy’s Bar n’ Grill in Broad Ripple with friends, the officer approached her stating she needed to give him the approved paperwork to validate her parking placard. When she responded that by law she wasn’t required to carry paperwork, but need only display the parking tag, the situation escalated, she said. Although Marsden’s friends viewed the encounter as the result of racial prejudice, she believes it reveals the bias some hold against those with hidden disabilities. “My friends were upset saying the officer didn’t want us there because we were Black, but I was convinced it was because he wasn’t clear I had a true disability,” said Marsden. “I had my purse so he coudn’t see my equipment. I told him I’m a heart patient and I have an LVAD and a pump attached to my heart. I raised my shirt and showed him my bandaging and driveline. As I go to pull out my batteries he said… ‘I need to see your paperwork.’” Marsden adds the officer stated, “you can park here, but you have to go home and get your paperwork first.” At that point, she knew she had been discriminated against, if not for racial reasons, but for her disability or gender. Seeking help The very next morning, Marsden sought out the BMV for clarification of her placard and paperwork. Although the staff said they have no knowledge of individuals needing to carry validation paperwork, when Marsden began to explain her interaction with the officer, she was immediately referred to the agency’s government hotline. “They’re (BMV) the government agency that approves and issues placards, so that should be common knowledge for them. I’m still unsure why they didn’t have a definite answer,” noted Marsden. From there, she submitted a 27-page citizen complaint complete with her medical history, a cover page, table of contents and an introductory page. “When I went to the Citizen’s Complaint Review Board, the receptionist and the supervisor said they’ve never heard of an officer asking someone for paperwork. I requested the officer to be terminated, but at the very least demoted,” she said. Additionally she spoke with the FBI, the Indiana Civil Rights Commission and the U.S. Department of Justice in Washington, D.C. As a result of the situation being physically and emotionally draining, Marsden said she has now been diagnosed with post-traumatic stress disorder and placed on medication. The Recorder reached out to IMPD officials, but at press time, no statements were given. Life as an LVAD patient At all times, Marsden has the LVAD connected to her, along with two batteries—equipment which keeps her alive. It was July of 2002 when the then 28-year-old Marsden was caring for her two children, one only two months old, when she began experiencing extreme shortness of breath. The emergency room physicians said she had a touch of walking pneumonia. She was given medicine and told not to return for three days to allow the medicine to begin treatment. “The second day I called a friend and said ‘I need to go back because if I go to sleep, I’m not going to wake up.’” Chest X-rays revealed she had congestive heart failure and a hole in her lungs. She was placed in the Intensive Care Unit for 10 days and was officially diagnosed with PPCM. During pregnancy, changes occur within the heart and blood vessels which may put extra stress on a woman’s body. The National Institute of Health said “PPCM is often not diagnosed until late in its course, because its clinical manifestations are highly variable and a heart disease may not be suspected at first. Frequent presenting symptoms of PPCM, such as prostration, shortness of breath on mild exertion, and coughing, are often initially misinterpreted as evidence of pneumonia or as physiological accompaniments of pregnancy and delivery.” Unlike an artificial heart, an LVAD doesn’t replace the heart, it simply assists the heart in performing its normal functions. It is usually used for those whose heart needs rest after open-heart surgery or someone awaiting a transplant. Since Marsden was once diagnosed with stage one lung cancer, she is unable to be listed for a heart transplant until she has been cancer free for five years because some antirejection medications cause cancer cells to grow and spread. Her medical challenges have left her vulnerable to the psychological stress she experienced during the encounter with the IMPD officer, stated Marsden. “Originally my LVAD was to be a bridge to my transplant, but now I’m afraid of the possibility of cancer,” she admits. “I’ve been through open heart surgery, lung cancer, six blood clots in my leg at once, but this has affected me in ways I couldn’t have imagined. It’s more than a violation, it’s like he took a part of me, and for what reason?” Some might think Marsden’s assertions of psychological trauma are hard to understand, but she’s been informed it could literally have turned into a life or death situation. Recently, a medical professional explained to her that if the officer had grabbed her driveline the wrong way, not only would she experience excruciating pain, she could die. This brought about a fear Marsden never realized she had. “I wanted doctors to remove it (LVAD),” stated Marsden. “I’ve been comfortable with this for the past three years and doctors sat and talked to me to say, I can’t survive without it. From there I couldn’t get out the bed because I was paranoid and depressed.” Eddie Journey of Goodpoint Counseling & Consulting Services LLC said instances like this can take an individual on a distressed emotional journey. “Part of it is an identity issue and the difficulty is when others take it upon themselves to define your identity for you,” said Journey. “People don’t have a right to your public health information and it’s problematic when you feel as if you have to disclose it in order to gain what’s right.” The face of disability Deb Hileman, executive board member of the Invisible Disabilities Association Board said 80 percent of people with disabilities and qualified to use handicapped parking spots do not use a wheelchair or walker. “The people that talk to us say it’s very distressing and discouraging that they have to show their scars to prove they can use a parking space. Our association tries to educate the public to understand ‘just because you can’t see it, doesn’t mean it’s not there.’” Invisible disabilities include lupus, sickle cell anemia and fibromyalgia among several others. Recently a story of a woman with fibromyalgia, a chronic disease that causes pain, fatigue and muscle stiffness, has received national attention after she parked her car in a handicapped spot and found a note on her window. The note, discovered by her son read, “Being fat and ugly doesn’t count as disabled – park somewhere else.” “As a society we’ve gotten out of control with judging people based on their looks,” believes Marsden. “You can’t look at someone and determine what’s wrong with them or what they’re going through. You don’t know my story just by looking at me.” Marsden wonders if she would’ve received different treatment if she were an elderly white woman in a wheelchair or with an oxygen tank. Previously, she didn’t talk about her disability, so revealing it has been challenging. She said she’s even been criticized for looking her best. “But why shouldn’t I look good? I don’t do that for other people, I do that for me because it helps recovery,” she commented. “Just because I’m ill on the inside doesn’t mean I have to look like it.” Hileman believes as the baby boom generation ages, as more people are living longer but not necessarily healthier, more will struggle with invisible disabilities. She also mentioned handicapped parking wasn’t available when she was growing up. “Now we have them more and more and they’re usually full but it’s going to become an increasing challenge because there aren’t enough of those spaces out there,” she said. Gaining community support Two petitions have been created on MoveOn.org by Marsden, one to highlight the civil discrimination situation and another addressing hate crimes. “Everyone I’ve talked to about the situation said they commend me for taking a stance because we talk about everything (police) do to us but we don’t come together as a community. What happened to me leads to Ferguson and Baltimore,” she stated. Her biggest priority is gaining community support with at least 1,000 signatures. Currently about 160 individuals from 32 states and four countries are in support. She was also encouraged when the owners of D & C Pizza showed her support. The business has agreed to spread awareness by placing information about Marsden’s incident and petition information on all of their pizza boxes. “People don’t realize how often this happens because it goes unreported. Some people are just scared because they are afraid of retaliation. I’m not afraid, because if you come after me, I’m going to come back after you even harder,” said Marsden. “We have to stand up as a community.
DISABILITIES HAVE ‘NO FACE,’ THOSE AFFLICTED FIGHT FOR CIVIL RIGHTS
By VICTORIA T. DAVIS @Victoria08Davis | Posted: Thursday, May 14, 2015 10:19 am
How would VAD patients feel about the prospect of totally internal implants with no external driveline or electrical supply? Would you feel insecure or nervous about not having your supply source outside your body? Here’s an interesting article about another wireless implant that is being developed.
Another LVAD Company Joins Quest for Fully Implantable System
ReliantHeart announces a partnership with Dualis MedTech to create a wireless LVAD that uses transcutaneous energy transfer.
ReliantHeart is working to make its HeartAssist5 fully implantable.
Over the past few years, giants in the field of left ventricular assist devices (LVADs) Thoratec and HeartWare have both discussed efforts to create an LVAD that can be implanted completely within the body, eliminating the need for an external driveline. Now, ReliantHeart, a Houston, TX-based company that makes the HeartAssist5 (HA5) LVAD, has announced a partnership with Dualis MedTech GmbH to develop a fully-implantable LVAD.
The HA5 has CE Mark approval and is being studied in an FDA trial. Under the partnership, Dualis will integrate its MedBase wireless energy transfer technology with the HA5 LVAD, forming a system that uses less than half the energy of other full flow LVADs, according to a press release.
The MedBase technology will also be used to create a wireless, fully-implantable LVAD that is powered by magnetic coils inside and outside the body. This wireless system is slated to be available in 2016, according to ReliantHeart. What’s more, patients with a HA5 will be able to get rid of their external drivelines and upgrade to the wireless system without having to change out the heart pump.
Dualis, which was spun out of the German Centre for Aeronautics and Aerospace (DLR), has been developing the MedBase technology since 2006. Dualis chief executive officer Stephan Sagolla said in a press release, “The internal coil is about two inches in diameter and will communicate with an internal battery and power management much like a pacemaker system. The patient will be wireless.”
A fully implantable LVAD has long been the goal for this therapy. LVADs have allowed patients to enjoy relatively high survival rates and more active lifestyles, but driveline infections, often around the area where the power driveline exits the patient’s body, have been a somewhat frequent adverse event. Showering, swimming, and water-related activities remain difficult for patients because of the use of external power.
ReliantHeart has been working with Dualis and a number of other companies to improve the LVAD technology. Rodger Ford, ReliantHeart chief executive officer, said in a press release, “Our mission is to compress time and accelerate beneficial outcomes. Artificial heart pumps need power but running wires through the skin leads to infection and patient discomfort. The solution is to invent a device to transfer power without wires.”
The company also recently announced a partnership with Kollmorgen Corp. to reduce HA5 power consumption by 50% with an energy efficient motor stator. The announcement explained that energy efficiency would help achieve the goal of a wirelessly-powered LVAD.
Destination LVAD Devices Come With Caregivers’ Concerns and Tensions
Posted on
MedicalResearch.com Interview with: Colleen K. McIlvennan, DNP, ANP Assistant Professor of Medicine
University of Colorado, Division of Cardiology
Section of Advanced Heart Failure and Transplantation
Medical Research: What is the background for this study?
Response: Destination therapy left ventricular assist device (DT LVAD) patients are often older with significant comorbidities that preclude heart transplantation. As such, the decision to get a DT LVAD is arguably more complicated than the decision to receive a temporary LVAD in anticipation of a transplant. Centers offering LVADs often require the identification of a caregiver prior to proceeding with the implant. Caregivers are commonly female spouses of DT LVAD patients, who are also older with co-morbidities. Understanding their perspective in DT LVAD decision making is extremely important as they are at particular risk for experiencing stress and caregiver burden due to the increased demands on caregiving with DT LVAD.
Medical Research: What are the main findings?
Response: We performed semi-structured qualitative interviews with 17 caregivers: 10 caregivers of patients living with DT LVAD, 6 caregivers of patients who had died with DT LVAD, and 1 caregiver of a patient who had declined DT LVAD. Throughout the interviews, the overarching theme was that considering a DT LVAD is a complex decision-making process.
Additionally, three dialectical tensions emerged:
1) the stark decision context, with tension between hope and reality;
2) the challenging decision process, with tension between wanting loved ones to live and wanting to respect loved ones’ wishes; and
3) the downstream decision outcome, with tension between gratitude and burden.
Medical Research: What should clinicians and patients take away from your report?
Response: Several interventions should be considered for caregivers of patients considering DT LVAD.
First, in order to better prepare caregivers for the burdens of DT LVAD, LVAD programs should continue to invite caregivers to participate in the decision-making process. This helps to address caregivers’ concerns and works to further engage them as active participants.
Second, DT LVAD caregiver-specific tools and resources should be developed to outline responsibilities and the impact on the caregiver’s life.
Third, providing caregivers with tools such as a decision aid may help to manage expectations and relieve the potential for post-decision caregiver burden. It is important for programs to normalize the ambivalence felt by caregivers by informing them that others have experienced this as a very complex decision.
Fourth, ongoing caregiver support groups, separate from patient support groups, can assist in empowering caregivers as well as validating feelings and concerns.
Medical Research: What recommendations do you have for future research as a result of this study?
Response: Future work surrounding caregivers of patients considering DT LVAD should explore the decision process prospectively. Additionally, future studies should investigate the potential correlations between caregivers and their propensity toward certain tensions (e.g. which characteristics make caregivers more likely to have decision regret). This would lend itself to identifying caregivers who would benefit from tailored caregiver support or interventions, with some caregivers potentially needing no interventions at all.
Comments Off on Australians Develop First Bionic Heart
This world-first bionic heart works without a pulse
Human transplants are expected from 2018.
BEC CREW 11 MAR 2015
Australian researchers have invented a new type of bionic heart that pumps blood around the body without a pulse. Named BiVACOR, the device has been successfully implanted in a sheep, and works so well, researchers are hoping to run human trials in just three years. Not only does the device last for up to a decade, but it’s smaller, and less susceptible to wear and tear than current artificial hearts. “There were other devices that were quite large, and they also would break quite easily,” one of the team Daniel Timms, formerly from the Queensland University of Technology, told Jorge Branco at The Brisbane Times. “And the reason they would break is they would have a sac, so if you’re beating them billions of times per year, they’re going to break.”
BiVACOR is a relatively simple device, made from two titanium centrifugal impellers – or discs – placed on a single rotor. These discs spin together at 2,000 revolutions per minute to smoothly push incoming blood through the other end of the device, which is “a significant departure from traditional pulse-based designs, which included balloon-like sacs to pump blood”, says Branco. Because the device contains just one moving part – the rotating discs in the middle – there’s very little in it that can wear down and malfunction. The device was transplanted into a live sheep in January, and so far, so good. Just a little titanium disc spinning inside, keeping the sheep alive, most importantly, and also perfectly healthy. Here’s how it works:
“We’ve now shown that the device works. This idea is viable. Now it’s a matter of making it robust and reliable so that it works in a patient,” Timms told Branco. “The time frame is three to five years before it could be ready for humans. Proving the concept was the first real hurdle. There are many to go from here but we’re confident we have the collaborative team to take it to that next level.”
With heart failure affecting 300,000 Australians at any given time and 1.1 million people across the US and Europe, this is pretty exciting. Especially when you think about how just 4,000 donor hearts are available globally each year. We need something like this. Let’s see what the clinical trials bring.
Comments Off on Could LVAD’s Be Used to Prevent Heart Failure? One Study Says Maybe!
There is evidence that use of the #LVAD could actually help prevent heart failure.
A new study led by UT Southwestern Medical Center researchers suggests that the long-term use of left ventricular assist devices(LVAD) by patients who suffer from heart failure issues might induce the regeneration of heart muscles, as it prevents oxidative damage thanks to a cell-regulator mechanism.
LVADs are devices implanted in patients awaiting heart transplants; they are mechanical pumps that act as substitutes for the damaged heart, pumping blood throughout the body.
Dr. Hesham Sadek analyzed DNA markers of damage and cell proliferation in 10 patients, assessing them in pre- and post LVAD situations. The team based their study on previous data that demonstrated the capacity of newborn mice hearts to regenerate through activation of cell division. In this project, researchers showed that by assisting the damaged heart through LVADs usage, the oxidative stress of heart muscle cells would be alleviated.
Dr. Sadek commented in a press release: “We looked at markers of what is called the DNA damage response in cardiomyocytes (heart-muscle cells) of these patients. The response is composed of a cascade of proteins that is activated in response to DNA damage and in turn shuts off the ability of cardiomyocytes to divide. We found that patients who were on LVAD for more than six months had significantly decreased levels of DNA damage response.”
The research team found that those who used LVADs for six or more months had a 3-times higher rate of cardiomyocyte proliferation.
“This result shows that patients with mechanical assist devices have the ability to make their muscle cells divide. And the obvious question now is, ‘Are these hearts regenerating? Could LVADs be used as a cure for heart failure?’” said Dr. Sadek.
Dr. Pradeep Mammen, Associate Professor of Internal Medicine at UT Southwestern and co-senior author of the study, added, “Putting in a mechanical pump rests the heart and apparently sends a signal to make new heart cells. This is the first time that this phenomenon has been shown to occur in human heart failure.”
It is estimated that 6 million Americans live with high risk of heart failure, according to the American Heart Association. This incidence is expected to increase over the next 2 decades as the population ages and available treatments improve survival rates.
“This is an exciting advance. We have a long way to go, but hopefully this study will be an important first step (…),”concluded Dr. Mark Drazner, Professor of Internal Medicine and Medical Director of the Heart Failure, LVAD, and Cardiology Transplant Program.
Comments Off on The Truth About Insurance Coverage for VAD Driveline Supplies: What You Need to Know
The Truth about Insurance Coverage for VAD Patient Supplies
Decreasing the Risk of Financial Hardship for the VAD Patient at Home
Medicare guidelines – In 2012, CMS made the determination that traditional DME companies could no longer bill dressing supplies for VAD patients and that billing entities must have a “carrier provider” designation. Many DME companies do not know that the rules have changed and are still trying to bill some of the supplies. If a Medicare audit indicates that a DME has been billing and receiving reimbursement for VAD supplies, Medicare will most likely ask for repayment. Because such an event could cause a DME company to financially fail, the DME would likely bill the patient for the amount recouped by Medicare.
Commercial insurance – Traditional DME’s can bill for VAD patients having commercial insurance or Medicaid. However, hospital reliance on an insurance company’s short list of in-network DME suppliers for outpatient driveline dressing supplies can be a costly mistake. Unfortunately, insurance companies rarely know the limitations of their chosen and usually, long-standing DME suppliers. The truth is that traditional DME suppliers are often unfamiliar with the unique needs of VAD patients and many times will substitute ordered products for inferior ones or different ones. This practice can ultimately put the patient’s health at risk. Updates on new, possibly better-qualified in-network providers for outpatient supplies are not always available to the hospital.
In many cases, insurance companies will see the need for a niche provider and allow it into their networks to provide services for unique patients such as those with a VAD. A supplier company that has insurance company relationships and deals one-on-one with these companies daily can often convince a given insurance carrier to provide appropriate benefits and to even let them into network as a provider for future VAD supply claims.
VAD facilities should seek a VAD-knowledgeable company that understands the unique needs of these patients and that will research each patient’s specific policy benefits and discuss them with the patient before sending out VAD dressings and supplies. A knowledgeable company has the skill to advocate for the patient by fighting for patient coverage and the insurance carrier’s preauthorized, correct payment for VAD supplies. This can reduce the chances for unexpected, exorbitant patient copays.
Medicaid – Many DME companies do not attempt to become in-network providers in state Medicaid programs because reimbursements are not always sufficient and are slow to be processed.
It is illegal for a company to provide products to Medicare patients withot billing for them. This is considered an inducement and is deemed an unfair business practice under the law. Patients should receive statements from their insurance provider showing that billing has occurred. Providers are also required to make reasonable attempts to collect copay amounts
Comments Off on Close Friend Helps Man Prepare for #VAD Implant
Planning Ahead for a #VAD –
Friends Raise Funds for Westfield Heart Patient
Jill D’Ambrosio
Saturday, February 14, 2015 • 9:28pm
WESTFIELD, NJ – On Valentine’s Day, resident Doug Lynch has a message for the community: Please help in his effort to raise funds for his close friend, Dan Weiniger, a Westfield resident who is preparing for open heart surgery on Monday.
On Friday at 5 p.m., Lynch launched a fund drive on GoFundMe.com to raise money to purchase a whole house generator to be installed at Weiniger’s Westfield home. The fundraising goal is $8,736. By Saturday afternoon, over $1,200 had been donated.
The generator will provide a guaranteed source of electricity needed to recharge daily Weiniger’s new left ventricular assist device (LVAD), which will be implanted during Monday’s operation at Morristown Memorial Hospital. The LVAD will help Weiniger’s heart pump blood more effectively.
In the last few years, the region has lost power several times for prolonged stretches due to hurricanes and an ice storm. For this reason, the generator is crucial to Weiniger’s well-being.
“If the power goes out, it’s literally life and death,” said Lynch.
Fourteen years ago, Weiniger, now 53, underwent successful quintuple bypass surgery and was doing well until he suffered a heart attack last week, which caused severe damage to his heart.
“Dan is now in heart failure, and another bypass is not an option. Neither are new drugs or stents,” reads the statement on GoFundMe.com.
Lynch met Weiniger through Westfield’s chapter of Business Networking International, of which they have both served as presidents.
Weiniger, who is married to Jan and is the father of 14 year-old Eliza, owns and operates Home Video Studio in Westfield, where he specializes in transferring VHS recordings to DVDs.
“What he does is help families preserve their memories in a more permanent state,” Lynch said. “Dan is one of the kindest people I know.”
Lynch, who owns A-1 Basement Solutions in Scotch Plains, said that Weiniger is in the coronary care unit at Morristown Memorial awaiting surgery Monday.
“I consider it a great honor to do something for him,” said Lynch. “Also, I’d ask everyone who reads this to keep Dan in their prayers.”
TAP into your town! Get Your Town’s News In Your Inbox: Click here to sign up.
“Mechanical assisted circulation is the most rapidly developing area of cardiology, but there is no journal dedicated to papers in this area,” Dr. Guglin said. “The growing number of patients with heart failure, the limited pool of donors for cardiac transplantation, and several technological breakthroughs have all made the option of implanting a ventricular assist device as destination therapy more important, and therefore it’s essential to give cardiologists a dedicated forum to share their research and opinions on the topic.” A ventricular assisted device, or VAD, is an implantable device that helps the heart do its job when it is too weak or diseased to perform effectively on its own. Originally designed as a means to maintain circulation until a donor heart could be found, VADs are now gaining popularity as a destination therapy for patients with heart failure. The VAD Journal will be an open access publication, meaning that its content is available online without significant financial, legal or technical barriers. “We intend for the VAD Journal to be a forum where all subspecialties in the field of mechanical assisted circulation and advanced heart failure can share ideas and opinions,” Dr. Guglin said. “It was created with the purpose of enabling rapid dissemination of unbiased reviews of new findings and ideas for all interested parties.” The VAD Journal can be accessed athttp://uknowledge.uky.edu/vad/
“Mechanical assisted circulation is the most rapidly developing area of cardiology, but there is no journal dedicated to papers in this area,” Dr. Guglin said. “The growing number of patients with heart failure, the limited pool of donors for cardiac transplantation, and several technological breakthroughs have all made the option of implanting a ventricular assist device as destination therapy more important, and therefore it’s essential to give cardiologists a dedicated forum to share their research and opinions on the topic.”
A ventricular assisted device, or VAD, is an implantable device that helps the heart do its job when it is too weak or diseased to perform effectively on its own. Originally designed as a means to maintain circulation until a donor heart could be found, VADs are now gaining popularity as a destination therapy for patients with heart failure.
The VAD Journal will be an open access publication, meaning that its content is available online without significant financial, legal or technical barriers.
“We intend for the VAD Journal to be a forum where all subspecialties in the field of mechanical assisted circulation and advanced heart failure can share ideas and opinions,” Dr. Guglin said. “It was created with the purpose of enabling rapid dissemination of unbiased reviews of new findings and ideas for all interested parties.”
Comments Off on Clever HeartMate II VAD Recipient Alters Clothes to Fit Lifestyle
Ciera Stanley doesn’t let her HeartMate II LVAD stop her from looking fashionable. After receiving her implant in December of 2013, the twenty eight year old developed an ingenious method of modifying her clothing that allows for and hides the equipment that keeps her heart pumping.
Her inspiring story: “In December of 2008 I was attending school in western Maryland when I noticed I was having trouble walking up hills and getting to class in the cold weather. I thought I had asthma when I went to the campus health center and was directed to the emergency room at the nearest hospital in Cumberland. At this point it was believed that I had pneumonia or double pneumonia. After negative lung biopsies it was assumed that the problem was my heart so I was sent back home and admitted to Johns Hopkins where I was diagnosed with viral cardiomyopathy. From then on I had regular cardiology appointments, and my symptoms were mostly kept at bay by diet, exercise and medicines. Due to my tachycardia I had a pacemaker/defibrillator implanted in 2009. For the most part I lived fairly normally for a 23 year old, and for the next few years everything was under control.
In September of 2013 I began feeling short of breath and would have to stop frequently when walking for work or commuting. Using stairs was always daunting, but it was manageable. I was moving slower and slower, and Halloween night of 2013 I could not sleep lying down. I was only comfortable sitting straight up because there was so much fluid on my chest. That night I went into the ER for help and was hospitalized. After a months stay I was informed that I would need either an LVAD or a new heart. I was discharged but returned two weeks later and stayed for another two months awaiting my surgery.
I received my Heartmate II pump at Johns Hopkins on Dec. 20, 2013 and was discharged from the hospital two weeks later. The whole time I was in the hospital I stayed pretty upbeat, choosing to focus on the positive and making jokes rather than let my situation get me down. After a month and a half of recovery, I got back to most of my daily activities including socializing with friends, going to church and even dating. As a 28 year old I’d rather have my wires tucked away when out on a date, so I have employed the use of over sized bags just like ones I had owned before, but this time they are filled with my batteries and my controller. On days when I am just running errands or hanging with friends and don’t have to worry about my wires being compromised, I simply wear my batteries on my waist along with my controller. For the most part people don’t really notice them or ask me about them and are completely shocked when I explain what they are. For me, dressing the way I dressed pre-vad keeps me sane.”
Comments Off on Heart pump allows Salem man to live life, help others
Dave
A go-bag is something you pack with essential items and keep ready for use in the event of an emergency.
Dave Disselbrett has a slightly different definition.
His go-bag is something he grabs every time he leaves the house, whether it’s to go to a restaurant or to a woodcarving class.
Packed inside the black nylon bag, which looks a lot like camera bag, is a backup set of equipment for his heart pump, including an external controller and two power packs.
Disselbrett, 69, wears his heart on his shoulders. He has a harness with straps that go under his arms and holster-like compartments on each side for the power packs.
It is the uniform of a patient with a left ventricular assist device, or LVAD. While it may look cumbersome to others, for Disselbrett it’s about as comfortable as wearing a vest and as routine as putting on a pair of socks.
“I feel more out of place when I have my (woodcarving) apron on,” said Disselbrett, who lives in northeast Salem.
Several of his carving cohorts have been trained on what to do if his equipment malfunctions. A power pack can last up to 16 hours but when it falls below 20 percent, it begins to chirp loudly like a smoke detector in need of a new battery.
Chest compressions would be a paramedic’s first instinct, because Disselbrett has no pulse. But compressions could dislodge the device that is sutured to his heart.
Disselbrett’s pulse is undetectable — without a special Doppler blood pressure monitor — because the LVAD makes blood flow like water from a garden hose. He also doesn’t have a heartbeat that goes thump-thump. Instead, there’s a whirring or humming sound. Disselbrett described it like a bunch of bees buzzing.
Sharing his gift
Disselbrett has been hand-carving wood since he was teenager. His first projects were neckerchief slides for scouts. Now he carves mostly animals and small caricatures that are 4-5 inches tall.
You might have seen his work, including bears, pigs, bunnies, ducks and beavers, in the Artisan’s Village at the Oregon State Fair, where he has had a booth for years.
Disselbrett usually carves several of each animal with slight variations, whether that be in the actual carving or in the painting. Many are wearing clothing, including suits and ties.
“I don’t claim to be the most creative person in the world,” he said. “It does not bother me to do the same thing.”
He sells his carvings for $20 apiece, which means he probably makes $2 to $3 an hour, or just enough to cover the cost of his wood and tools. He uses basswood, the same kind of wood that was and still is used to create figures for Salem’s Riverfront Carousel, which opened in 2001.
“I wasn’t able to be involved because I had this thing called a job,” he said.
Disselbrett is a retired lumber broker who worked from his home office for a company out of New York.
Since retiring, he has had more time to carve and share his hobby with others. He teaches classes locally on Monday nights (Keizer Art Association) and on Wednesday mornings (Center 50+). He also teaches one afternoon a week in Beaverton and once a month in Eugene.
Around this time of year, he carves a lot of Santas and Christmas ornaments. He donates many of the ornaments to fundraisers that benefit the Capitol Woodcarvers, of which he is an active member.
Many of his woodcarvings also wind up as gifts for family members, friends, and even for his doctors and nurses.
Heart of a pioneer
Disselbrett is under the care of a seven-person team at Kaiser Permanente Sunnyside Medical Center in Clackamas. His surgeon, four doctors and two nurses all have extensive collections of his carvings.
“They are all over Kaiser, wherever you look,” said Barbara McKenna, RN and LVAD program manager. “He just gave me one for my first grandchild, a baby sneaker. It’s very sweet.”
The first one he gave to her was a bear in a white coat holding a sign that says: “I’m your new best friend.”
That was McKenna’s message to Disselbrett when they first met before he had the LVAD implanted in 2012.
Disselbrett was the recipient of Sunnyside’s first LVAD, and the surgery drew a crowd. His son has a photograph that shows 17 medical professionals in his room.
“I wasn’t really scared,” Disselbrett said. “I thought, ‘This can’t go wrong when you have everybody in the world looking at you.’ “
Kaiser currently manages eight LVAD patients and estimates there are about 100 LVAD patients overall in Oregon and 13,500 in the United States.
Traditionally, an LVAD is a bridge to a heart transplant. Disselbrett said he isn’t a candidate for a transplant. His heart still works, although not very efficiently. In his case, the LVAD is considered what McKenna called “destination therapy.” Those patients have a LVAD for the rest of their lives.
Plugged in 24-7
Disselbrett’s heart problems began in 1997, when he first had bypass surgery. In 2011, he had a massive heart attack at home. Although he called 911, he remembers little until eight days later when he woke up in the hospital. He was told his heart had to be shocked back into normal rhythm six times.
A defibrillator was implanted, and doctors warned him that he would eventually need something else done as his congestive heart failure worsened.
His heart was working at 30 percent capacity and struggling to pump blood to his extremities. His legs hurt so badly that walking to the mailbox was difficult and walking upstairs was nearly impossible.
He originally met with a heart transplant team but was ruled out. That’s when he was recommended for an LVAD, a mechanical pump that helps the heart move blood from its lower chamber to the rest of the body.
The device, about the size of a fist, and its connectors are implanted during open-heart surgery. One end is hooked with a tube to the left ventricle and the other with a tube to the aorta.
“They looked like garden hoses,” Disselbrett said.
Another tube passes from the device under the skin and out the abdomen. Disselbrett nonchalantly pulled up his shirt to reveal the dressing that he has to change weekly. The end is plugged into the controller, which also has plugs for each power pack.
The cords dangle noticeably below the hem of his shirt, so it’s obvious he’s plugged into something. But he said he doesn’t get many questions.
“I think most people are plain afraid to ask,” he said.
He has four sets of power packs, including the one he keeps in his go-bag. He charges them at night while he plugs directly into a large power unit that sits next to his bed. He said Kaiser notified PGE, his electric utility company, to place him on a list for priority power restoration in the event of a power outage.
Being an ambassador
Traveling can be a hassle, but Disselbrett has been to Alaska to go fishing with his son and to Montana to teach carving classes. Each time he called ahead to inform TSA of his travel plans, and each time he received royal treatment.
He wears a medical identification bracelet noting that he is diabetic, has an LVAD and cannot have CPR. His nurses are on-call 24-7 if there’s ever a problem.
“They want to know if this thing burps,” Disselbrett said.
He has an appointment with his doctors every six weeks, and also attends support group meetings every quarter and is routinely asked to meet one-on-one with LVAD patients or new candidates.
“He’s always available,” McKenna said. “He was the first implant at Kaiser, so we have a fondness for David and who wouldn’t? He’s such a beautiful person. He’s kind of our unofficial spokesman.”
Traveling can be a hassle, but Disselbrett has been to Alaska to go fishing with his son and to Montana to teach carving classes. Each time he called ahead to inform TSA of his travel plans, and each time he received royal treatment.
He wears a medical identification bracelet noting that he is diabetic, has an LVAD and cannot have CPR. His nurses are on-call 24-7 if there’s ever a problem.
“They want to know if this thing burps,” Disselbrett said.
He has an appointment with his doctors every six weeks, and also attends support group meetings every quarter and is routinely asked to meet one-on-one with LVAD patients or new candidates.
“He’s always available,” McKenna said. “He was the first implant at Kaiser, so we have a fondness for David and who wouldn’t? He’s such a beautiful person. He’s kind of our unofficial spokesman.”
Comments Off on HeartAssist5, The Smallest VAD of Its Kind, Implanted for First Time in Advanced Heart Failure Patient
CARDIAC SURGERY / CARDIOLOGY by EDITORS on Jun 30, 2014 • 12:34 pm
Left ventricular assist devices (LVADs) have come a long way in the last decade, keeping people with heart failure alive, including Vice President Dick Cheney, much longer than many thought possible. Not only have they been getting smaller, but they’ve been getting better at augmenting cardiac output while preventing clot formation. A new LVAD has hit the European market that’s smaller than any other and that has unique hemodynamic properties to optimize functionality for the benefit of patients. Last month ReliantHeart (Houston, TX) received the European CE Mark for its new HeartAssist5 pump and the device has just been implanted for the first time in a patient. It weighs only 3.3 ounces (92 grams) and features pulsatility transfer so that the blood vessels continue to feel a normal pulse generated by the heart itself. Perhaps more importantly, the HeartAssist5 pairs with the HeartAssistRemote Monitoring System that is capable of continuously sending patient data (direct blood flow measurement) to a cardiologist. The HeartAssist5 is still an investigational device in the United States and a U.S. trial is scheduled to begin later this year. Here’s an animation describing the implantation procedure for the HeartAssist5:






 e
e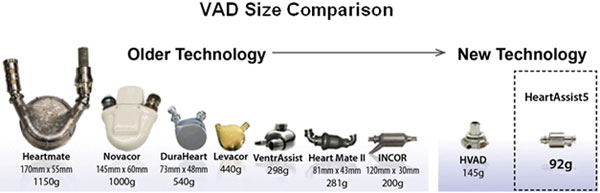
 Last month ReliantHeart (Houston, TX) received the European CE Mark for its new HeartAssist5 pump and the device has just been implanted for the first time in a patient. It weighs only 3.3 ounces (92 grams) and features pulsatility transfer so that the blood vessels continue to feel a normal pulse generated by the heart itself. Perhaps more importantly, the HeartAssist5 pairs with the HeartAssistRemote Monitoring System that is capable of continuously sending patient data (direct blood flow measurement) to a cardiologist. The HeartAssist5 is still an investigational device in the United States and a U.S. trial is scheduled to begin later this year. Here’s an animation describing the implantation procedure for the HeartAssist5:
Last month ReliantHeart (Houston, TX) received the European CE Mark for its new HeartAssist5 pump and the device has just been implanted for the first time in a patient. It weighs only 3.3 ounces (92 grams) and features pulsatility transfer so that the blood vessels continue to feel a normal pulse generated by the heart itself. Perhaps more importantly, the HeartAssist5 pairs with the HeartAssistRemote Monitoring System that is capable of continuously sending patient data (direct blood flow measurement) to a cardiologist. The HeartAssist5 is still an investigational device in the United States and a U.S. trial is scheduled to begin later this year. Here’s an animation describing the implantation procedure for the HeartAssist5: